
THE DIAGNOSTIC GAP: The ISS cannot tell if your brain is bleeding.
An astronaut lost the ability to speak for twenty minutes in orbit. Months later, no one can explain why. The real story is what that silence exposed about the architecture.

SUBJECT: CREW-11 MEDICAL EVACUATION // ISS DIAGNOSTIC ARCHITECTURE // DEEP-SPACE MEDICAL RISK
DATE: MARCH 29, 2026
CROSS-REF: THE PACIFIC DIVERSION | THE VERDICT | ANOMALY #45 (REMOVED)
DATA CONFIDENCE: VERIFIED (AP INTERVIEW, MARCH 28, 2026; NASA OCHMO-STD-100.1A; NASA SP-20240010473; NEJM 2019) + ANALYSIS (SENTINEL MEDICAL ARCHITECTURE REVIEW)

TWENTY MINUTES
On March 28, 2026, NASA astronaut Mike Fincke sat down with the Associated Press and told them what happened on the evening of January 7.
He was eating dinner. He had just finished prepping for a spacewalk the next morning. Then his voice stopped working.
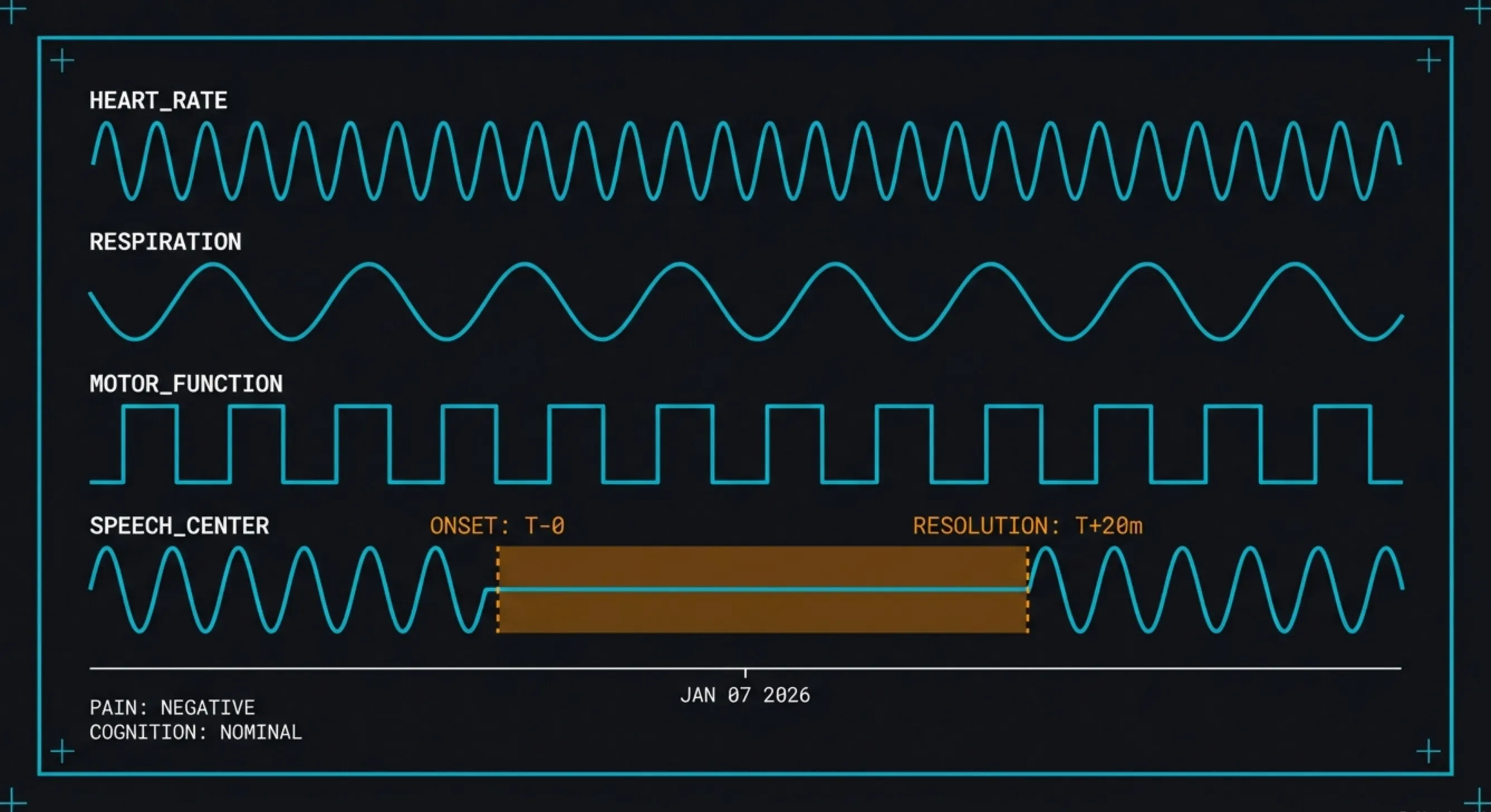
No warning. No pain. He was awake. He was aware. He knew he wanted to speak. He could not.
Twenty minutes later, it stopped. His voice came back. He felt fine. He has felt fine since.
His crewmates saw it immediately. All six people on the station gathered around him within seconds. Flight surgeons on the ground were contacted. The station’s ultrasound machine was pulled out.
The next morning’s spacewalk was cancelled. It would have been his tenth. It would have been Commander Zena Cardman’s first. Eight days later, all four Crew-11 astronauts were back on Earth, splashing down off the coast of San Diego more than a month ahead of schedule. They went straight to Scripps Memorial Hospital.
It was the first medical evacuation in the 25-year history of the International Space Station.
Fincke is 59. Retired Air Force colonel. Four-time space flier. He has spent 549 days in microgravity across his career. That puts him fourth on the all-time list for NASA astronauts.
Doctors ruled out a heart attack. He was not choking. Beyond that, they do not know what happened.
That was two months ago. They still do not know.
THE THREE GHOSTS
Here is the problem with diagnosing what happened to Fincke.
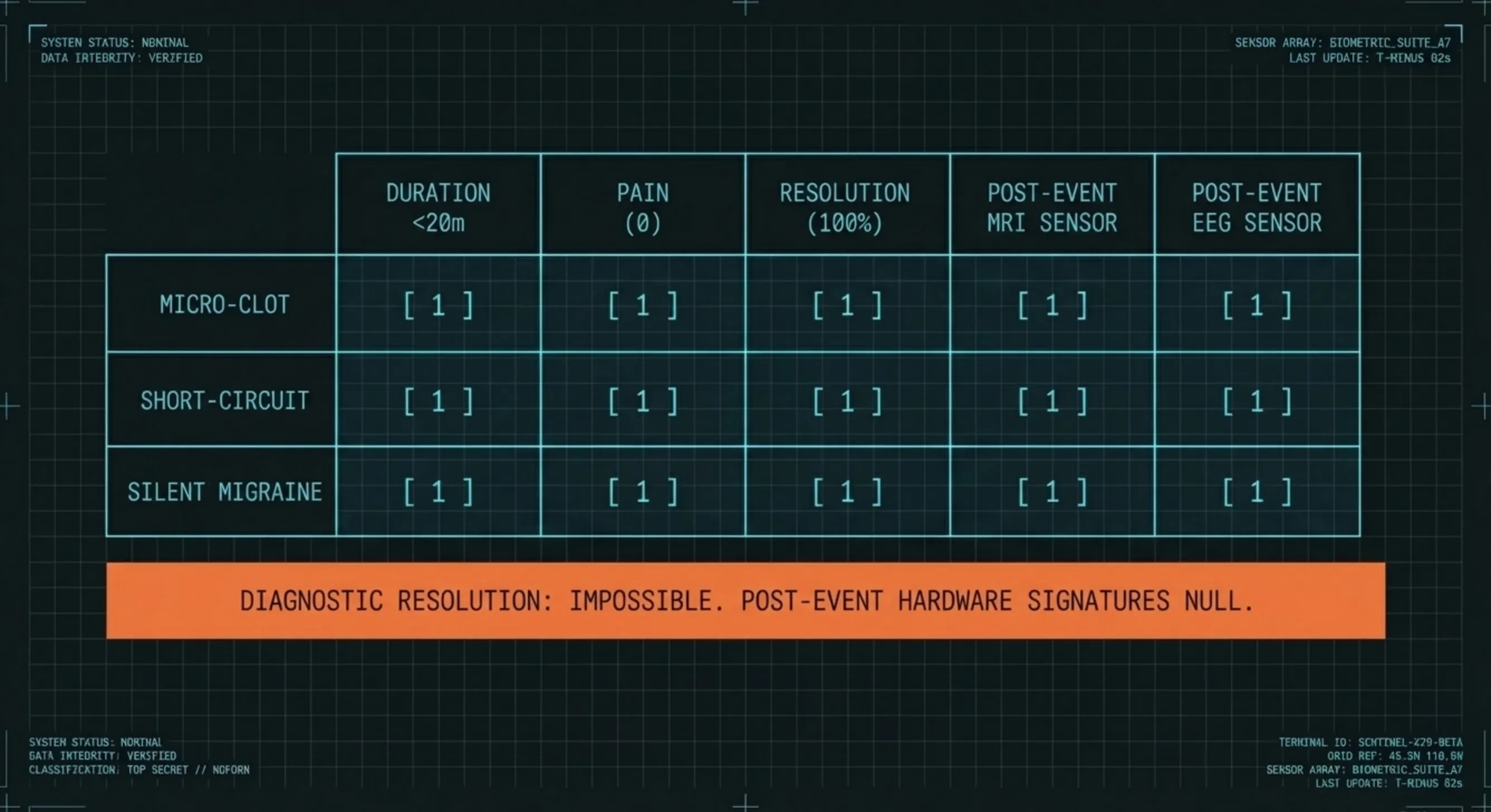
There are three conditions that match his symptoms perfectly. All three are well-documented in medical literature. All three are treatable on the ground. And all three are invisible by the time you get the patient to a hospital.
Think of it this way. You walk into a room and find a wet floor. No faucet running. No broken pipe. No rain coming through the window. The water is already evaporating. By the time a plumber arrives, the floor is dry.
That is what happened inside Fincke’s brain. Something interrupted the blood flow or electrical activity in the part of the brain that controls speech. Twenty minutes later, it fixed itself. By the time he was back on Earth and inside an MRI machine, there was nothing left to photograph.
The first candidate is a micro-clot. A tiny blood clot lodges in the artery feeding the speech center. Blood flow stops. Speech stops. The clot dissolves on its own. Blood flow returns. Speech returns. If the whole thing lasts less than twenty minutes, the brain tissue recovers completely. No damage. No scar. An MRI performed days later shows a perfectly healthy brain.
This is not a broken scanner. This is how these events work. The imaging is confirming that nothing was permanently damaged. It cannot confirm what caused the interruption, because the interruption is already over.
The second candidate is a short-circuit. A burst of abnormal electrical activity fires in the speech center. Not a full-body seizure. A localized one. The patient is awake, alert, and aware of everything happening around them. They just cannot speak. The burst itself might last seconds or minutes, but the brain needs recovery time afterward. That recovery period can stretch the total deficit to fifteen or twenty minutes.
An EEG performed days later will almost certainly be normal. Even in patients with confirmed seizure disorders, the tests between episodes are frequently clean. A single isolated event leaves nothing for the scanner to find.
The third candidate is a silent migraine. A wave of electrical suppression rolls across the speech center. This is the same thing that causes the zig-zag visual effects in migraine patients, except it hits the language region instead of the visual region, and it happens without a headache. It is a recognized diagnostic category. Duration: five to sixty minutes. Painless. Complete resolution. No trace on any scan. No blood marker. Nothing.
Twenty minutes fits all three. Painless fits all three. Complete resolution fits all three. Clean imaging afterward fits all three.
THE SENTINEL ASSESSMENT: The reason doctors cannot tell you what happened is not that they are hiding something. It is that the three most likely explanations are built to disappear. The condition resolves, and the evidence resolves with it. You cannot photograph something that is already gone. This is not a mystery of secrecy. It is a mystery of biology.
THE CHAIN
Now think about where this happened.
Fincke was not sitting in a restaurant in Houston. He was floating inside a pressurized aluminum can, 250 miles above the surface of the Earth, five and a half months into a mission, with 549 cumulative days of weightlessness on his body across four flights.
That changes everything.
In 2019, the New England Journal of Medicine published a finding that should have rewritten every spaceflight medical protocol on the books. An astronaut aboard the ISS had developed a blood clot in the jugular vein. The internal jugular. The main drainage pipe from your brain.
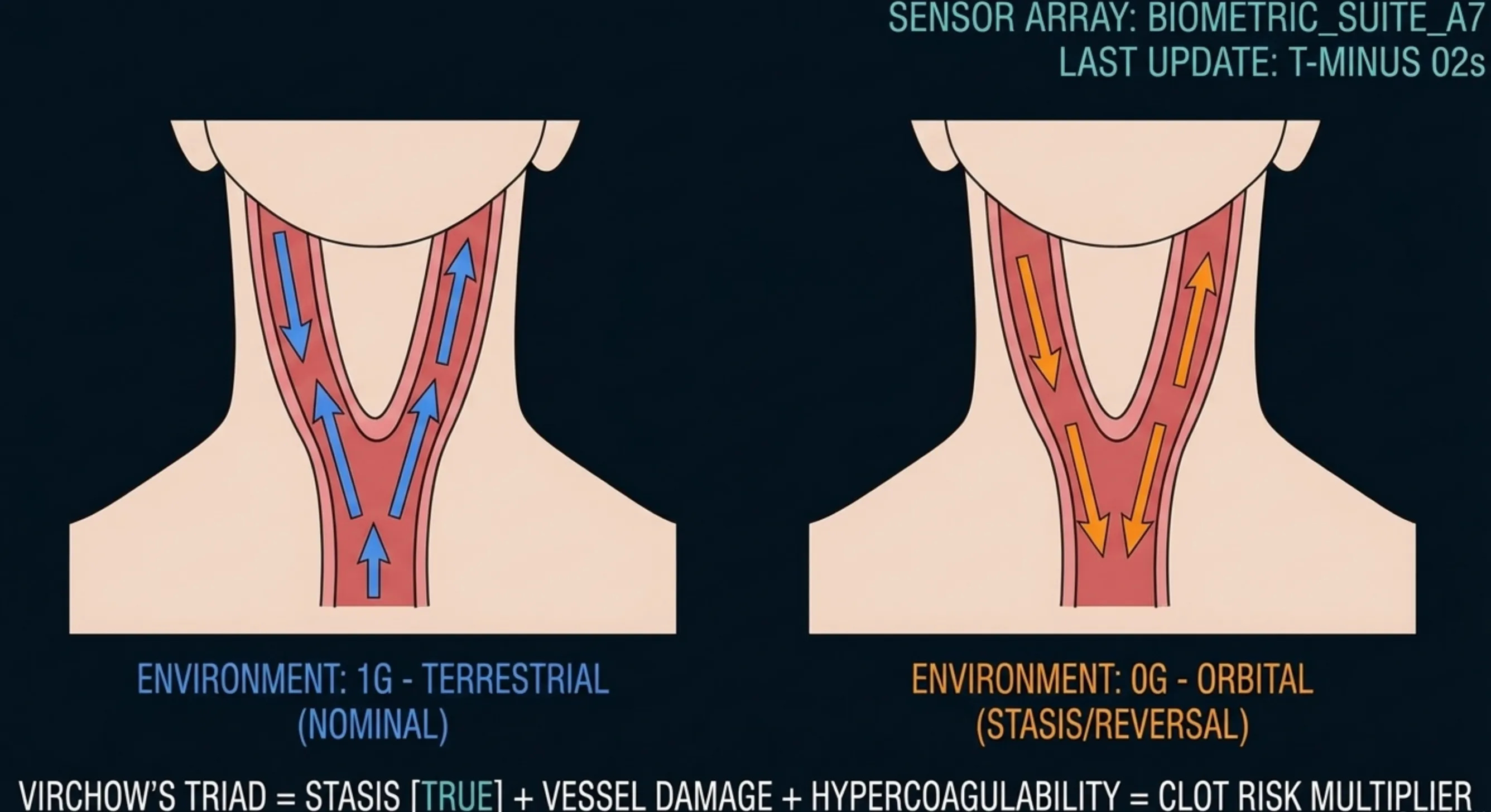
The research showed that microgravity fundamentally breaks how blood drains from your head. On Earth, gravity pulls blood downward. In orbit, it does not. The jugular veins swell. Blood flow slows. In some crew members, it stagnates completely. In some, it actually reverses direction.
Stagnant blood clots. This has been understood since the 1800s. There are three things that make clots form: blood that is not moving, blood vessels that are damaged, and blood that clots too easily. You only need one. Microgravity delivers the first one for free.
Now add the second variable.
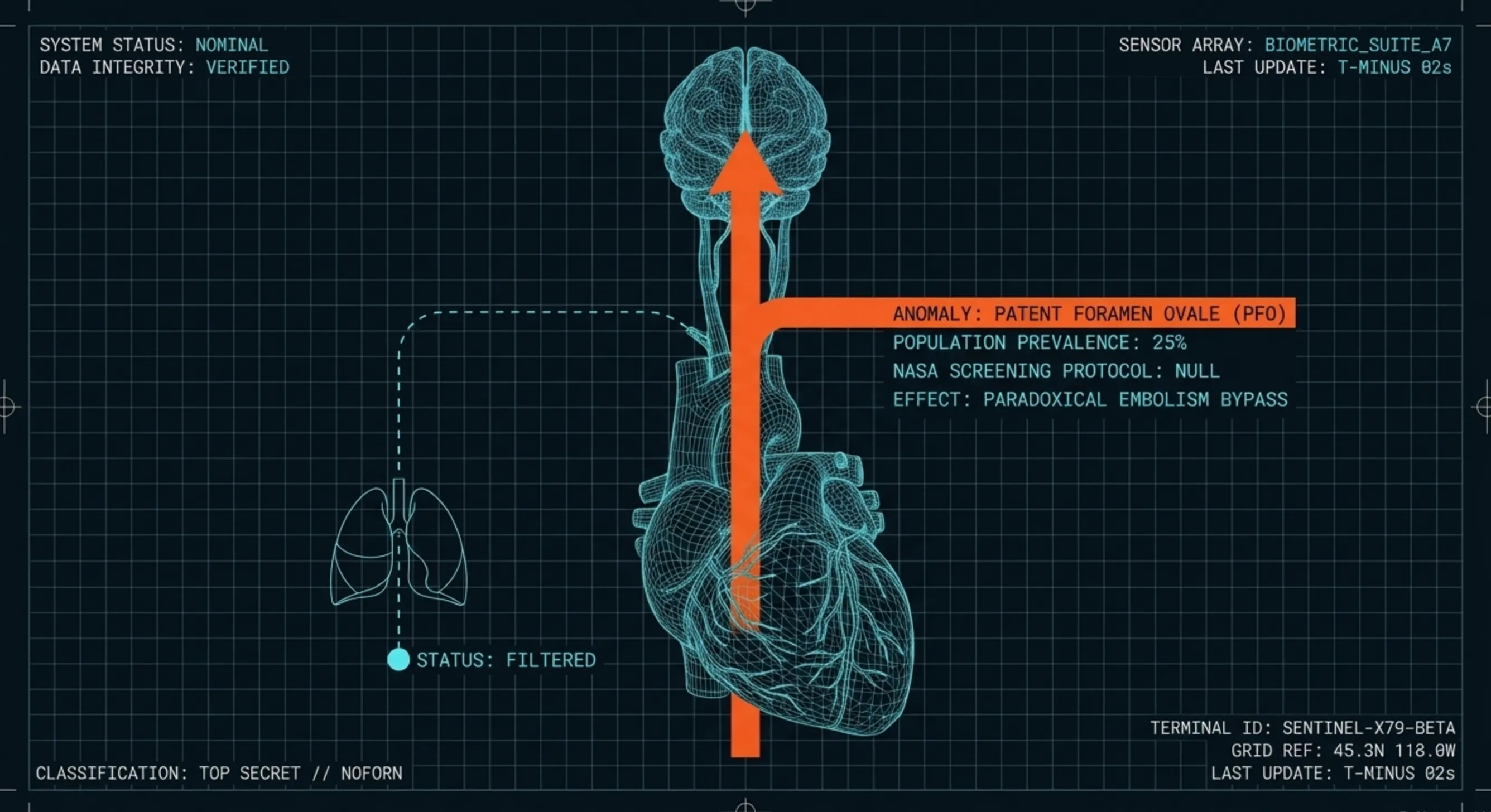
About 25% of adults walking around on Earth right now have a small opening between the left and right chambers of their heart. It is called a Patent Foramen Ovale. A PFO. It is left over from fetal development. Most people who have one will never know it exists. It causes no symptoms. It requires no treatment.
Unless you form a blood clot and it needs a way into your brain.
Normally, a clot in a vein travels to the lungs, where the capillary bed filters it out. That is the system working as designed. But a PFO creates a shortcut. A small clot can skip the lungs entirely. It crosses from one heart chamber to the other, enters the arterial system, travels up the carotid artery, and lodges in the brain.
This is called paradoxical embolism. It is the leading explanation for unexplained strokes in patients under 60 who have no risk factors.
Here is the institutional detail that matters.
NASA has never performed routine screening or evaluation for PFOs in astronaut candidates.
That is not speculation. That is NASA’s own language, from a 2024 OCHMO working group assessment. Under the current medical standards, a PFO only gets evaluated if it is discovered by accident or already known.
Read that again. One in four humans has a heart defect that creates a direct highway for blood clots to reach the brain. NASA sends humans into an environment proven to cause the exact kind of blood stasis that produces clots. And they do not screen for it.
Every link in this chain is documented. The venous stasis. The clot risk. The PFO prevalence. The paradoxical embolism pathway. The screening gap. Every single one has a published source behind it.
The only thing that is not documented is whether this specific chain fired in this specific patient on January 7, 2026. And it may never be. Because the evidence dissolved twenty minutes after it formed.
THE SENTINEL ASSESSMENT: This is not a conspiracy. It is a gap. NASA does not screen for a condition present in 25% of the population that creates a direct arterial bypass for blood clots, in an environment proven to generate blood clots. That gap did not matter when astronauts flew short shuttle missions. It matters now. At 549 days it matters a lot.
THE BLIND SPOT
When Fincke lost the ability to speak, his crewmates did everything right. They recognized it. They gathered around him. They contacted the ground. They deployed the station’s medical equipment.
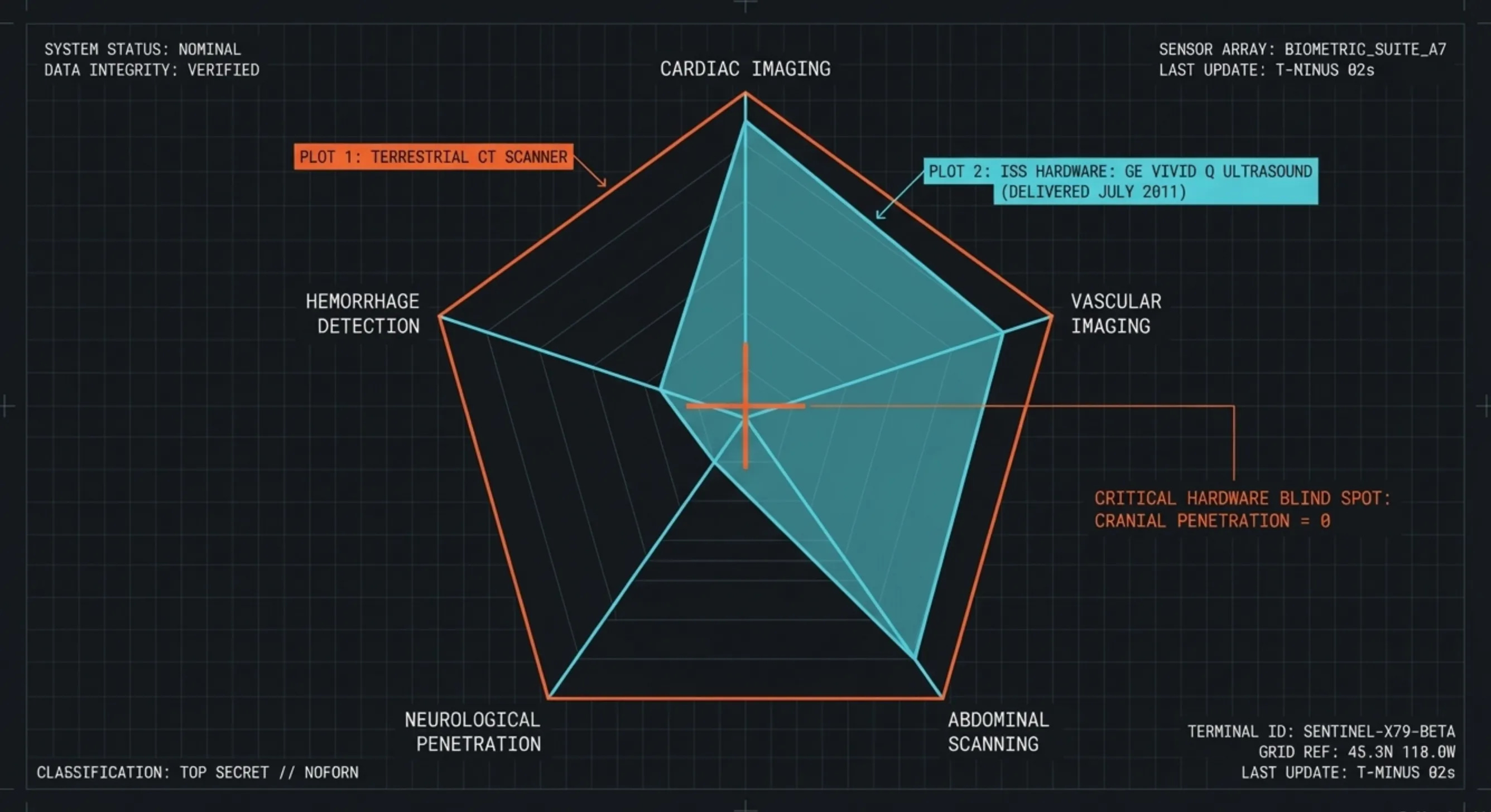
That equipment is a GE Vivid q ultrasound. It was delivered to the ISS aboard Space Shuttle Atlantis on July 8, 2011, during the final shuttle flight. It is a good machine. It can image the heart. It can check the jugular veins. It can scan the abdomen.
It cannot see inside the brain.
Sound waves do not penetrate the human skull with enough resolution to image brain tissue. The ISS has no MRI. No CT scanner. No way to look inside an astronaut’s head under any circumstances.
The flight surgeons on the ground were flying blind. They could check heart function. They could look at the jugular for clots. They could not determine whether Fincke was experiencing a dissolving blood clot, an electrical short-circuit, a silent migraine, or a brain bleed.
That last distinction is the one that kills you.
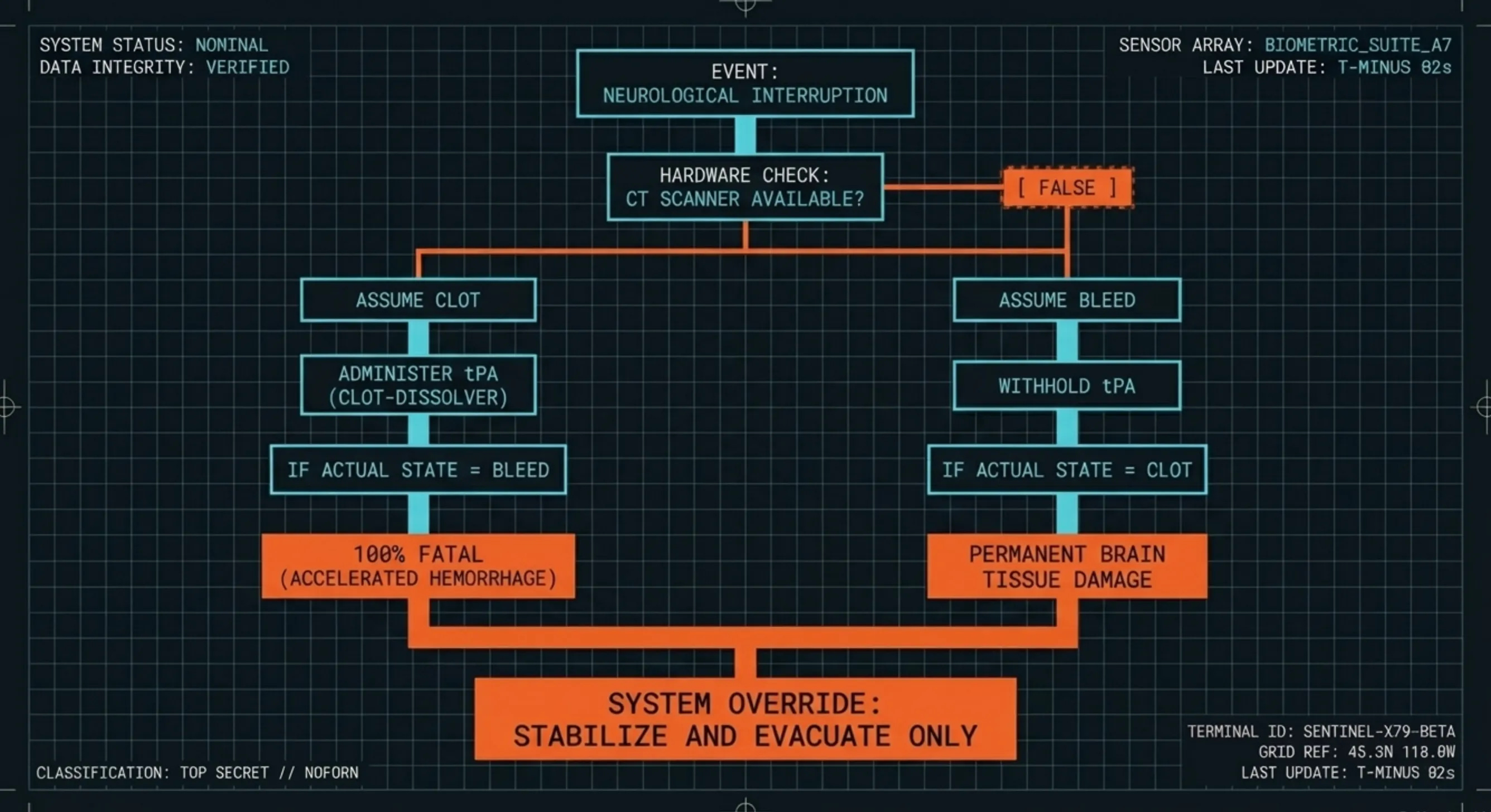
On the ground, when someone has a stroke, the first thing doctors do is a CT scan. Not to confirm the stroke. To answer one question: is this a clot or a bleed?
If it is a clot, you give a drug called tPA. It dissolves clots. It works. It saves lives.
If it is a bleed, and you give tPA, you accelerate the bleeding. The patient dies.
The entire treatment decision tree starts with a single scan. Clot or bleed. That scan takes minutes on Earth. The answer determines everything.
The ISS cannot perform that scan.
So the protocol for any suspected brain event on the station is: stabilize, do not give clot-dissolving drugs, and bring them home. That is exactly what they did. Dragon Endeavour undocked January 14. Splashdown January 15. Scripps Memorial Hospital within hours.
The system worked. The crew was flawless. The evacuation was controlled.
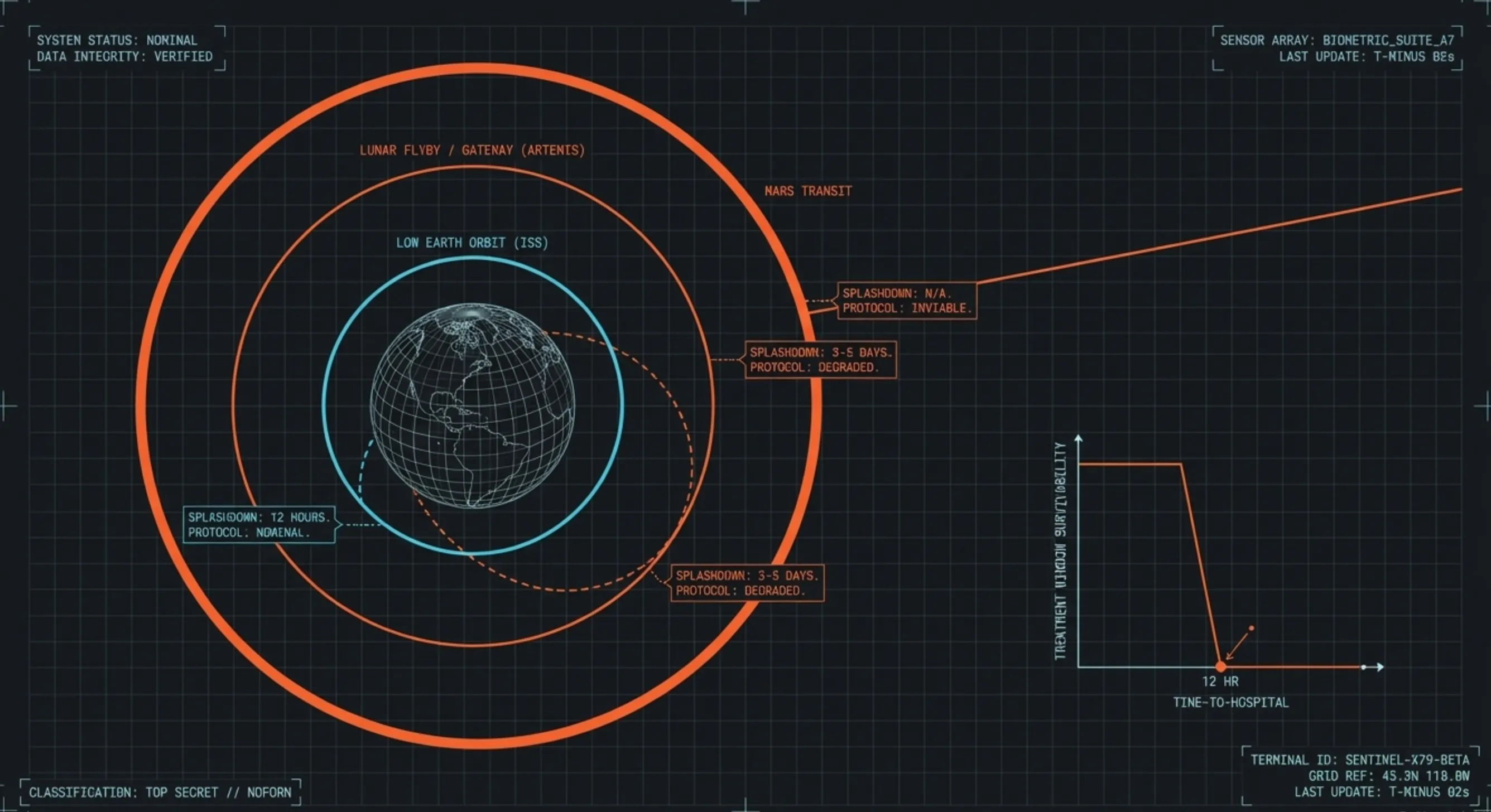
But the system only worked because Earth was twelve hours away.
THE SENTINEL ASSESSMENT: The ISS medical kit can keep you breathing. It can stabilize your blood pressure. It can scan your heart. It cannot answer the single most important question in stroke medicine: is this a clot or a bleed? Without that answer, the only safe protocol is evacuation. That protocol has an expiration date, and it expires the moment you leave Low Earth Orbit.
THE DISTANCE
The Artemis program is building toward sustained human presence on the Moon. Artemis II is targeting an April 2026 launch for the first crewed lunar flyby since Apollo. After that comes Gateway, the lunar space station. After that comes surface habitats.
If the same thing that happened to Fincke happens on Gateway, Earth is not twelve hours away. It is days away. The crew cannot just undock and fall home. They have to execute a translunar injection burn, coast for days, re-enter the atmosphere, and splash down. The patient has to survive the transit with whatever diagnostic tools are on board.
Those tools cannot distinguish a clot from a bleed.
If the same thing happens during a Mars transit, Earth is months away. Evacuation does not exist as a degraded option. It does not exist at all.
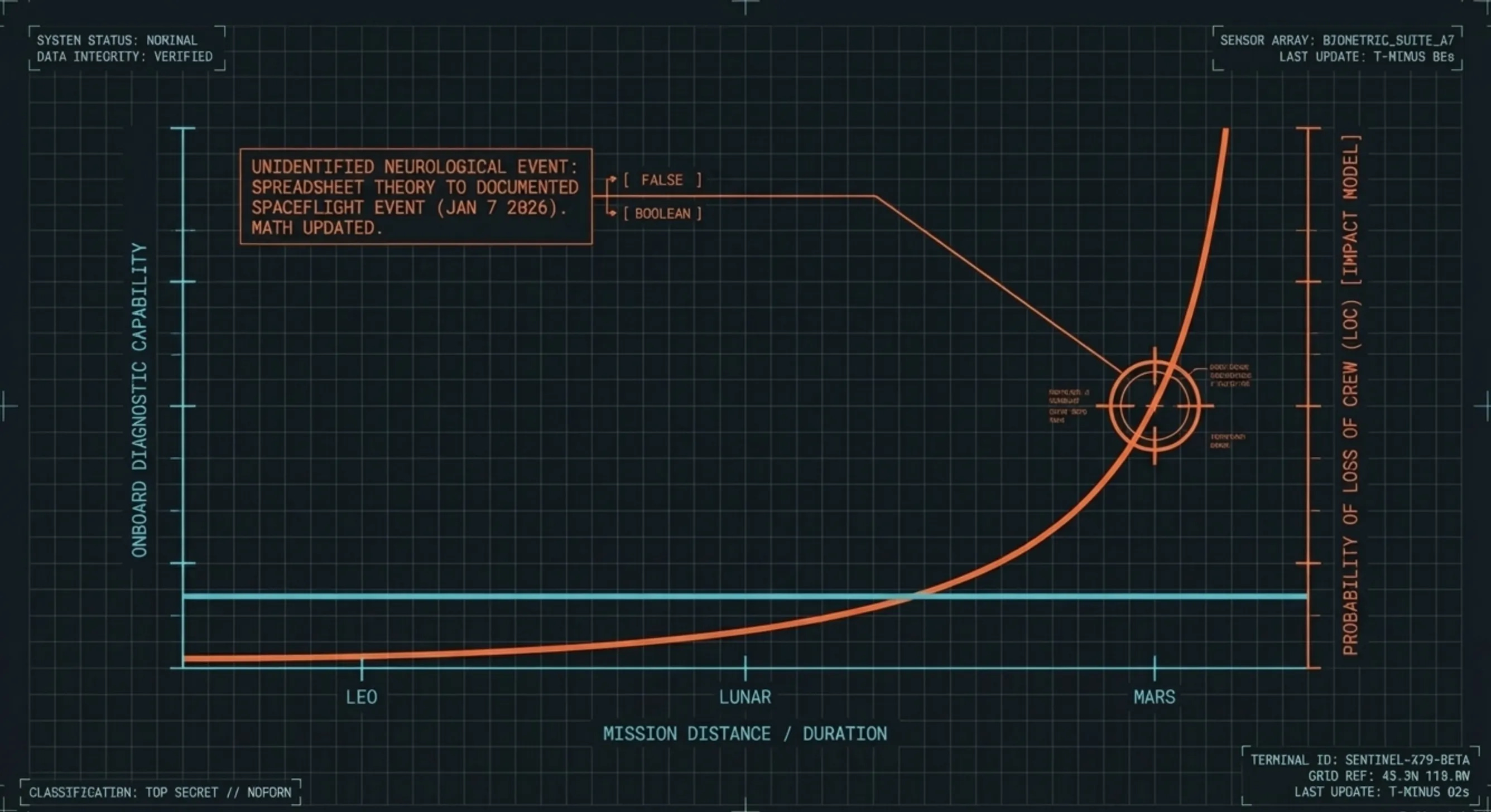
NASA models this risk. They use a framework called IMPACT that simulates medical emergencies across 119 conditions and calculates the probability of losing a crew member for each one. The Crew-11 evacuation just changed the inputs. A transient neurological event of unknown origin was a theoretical line item in a spreadsheet. Now it is a documented spaceflight event. It happened. The math has to update.
The gap is not in the crew. They responded in seconds. The gap is not in the protocols. The protocols worked exactly as written. The gap is in the hardware. The ISS medical suite can stabilize you. It cannot diagnose you. And until that changes, every astronaut who flies beyond LEO accepts a risk that cannot be identified, cannot be treated, and cannot be evacuated from.
THE SENTINEL ASSESSMENT: The ISS was never designed to be a hospital. It was designed to be a laboratory with a lifeboat. That assumption works in Low Earth Orbit, where the lifeboat reaches a hospital in twelve hours. It does not work at the Moon. It does not work at Mars. The next transient neurological event in deep space will not end with a controlled splashdown off San Diego. It will end with a crew making treatment decisions they are not equipped to make, about a condition they cannot image, with protocols that assume a hospital exists somewhere below them. It will not.
THE RECORD
A note on what we got right, what we got wrong, and what we are correcting now.
In January, we published SITREP: The Pacific Diversion, characterizing the Crew-11 splashdown trajectory as operationally anomalous. We framed the San Diego recovery as evidence of emergency routing. That framing was wrong. SpaceX transitioned to Pacific recoveries after Crew-10 due to trunk debris safety concerns. The splashdown location was standard. We corrected this in February. The correction stands.
Now we owe a second correction.
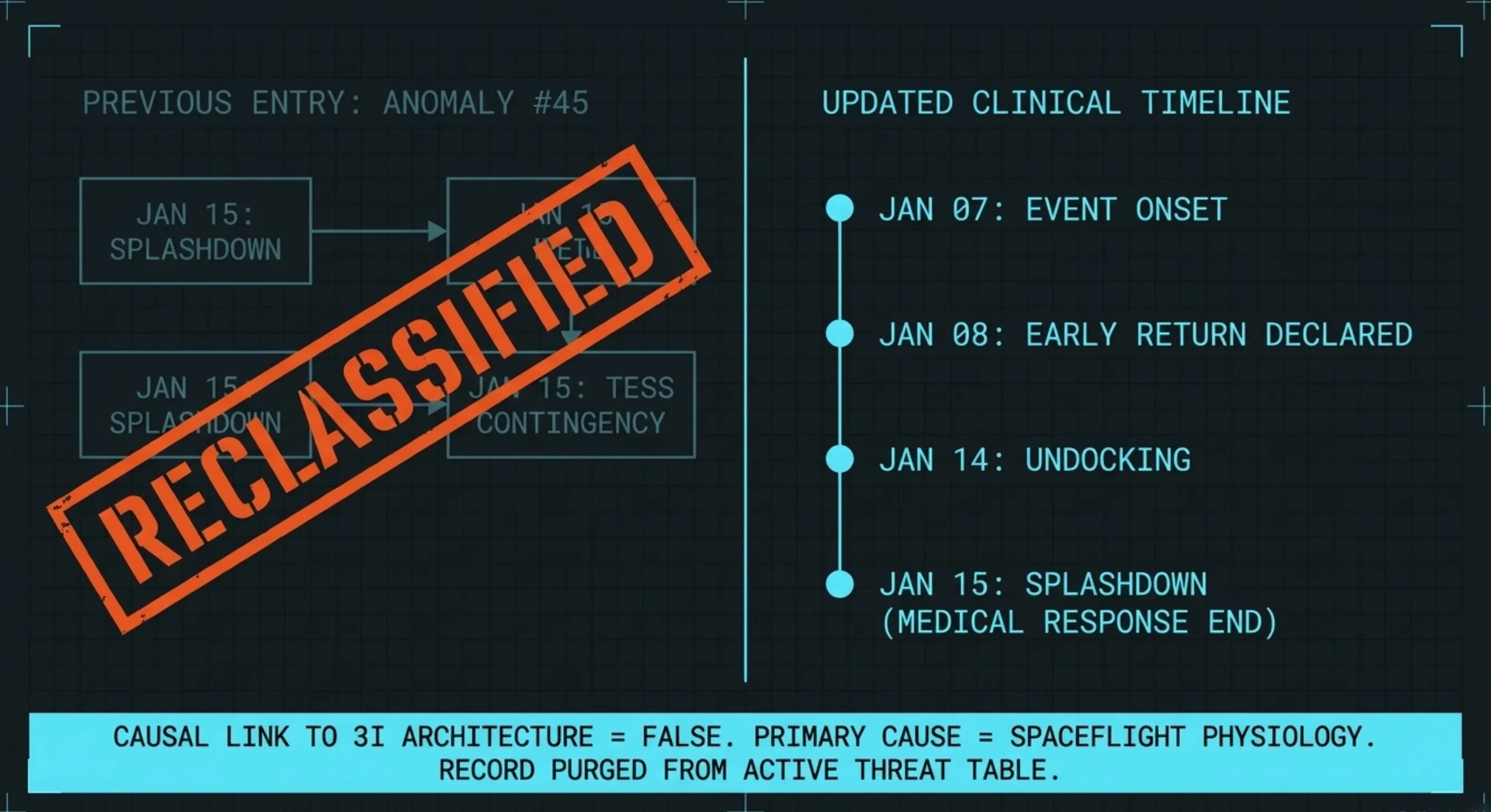
In THE VERDICT, we catalogued the Crew-11 evacuation as Anomaly #45 in the 3I/ATLAS anomaly table. The basis for inclusion was temporal proximity: the splashdown on January 15 occurred the same day TESS entered contingency mode. Two unprecedented events on the same day. At the time, we did not know what caused either one.
Now we know what caused the evacuation. Fincke’s neurological event occurred on January 7. NASA announced the early return on January 8. The undocking happened January 14. The January 15 splashdown was the end of a week-long planned medical response. It was not a reaction to anything that happened on January 15. The overlap with the TESS blackout is a scheduling artifact, not a signal.
The clinical picture confirms this. Every element of the causal chain connects to spaceflight physiology. Microgravity venous stasis. Cumulative exposure at 549 days. The PFO screening gap. None of it connects to 3I’s trajectory, emissions, or observation architecture.
Anomaly #45 is reclassified. It is removed from the active 3I/ATLAS anomaly table. The event is documented, not deleted. The Crew-11 evacuation happened, the medical mystery is real, and the ISS diagnostic gap it exposed is a legitimate finding. But it is a spaceflight medicine finding. It is not a 3I finding. Keeping it on the list would weaken the list, and we do not pad our numbers.
If we only reported findings that confirmed our prior conclusions, we would not be doing our job.
Fincke’s public self-identification in February and his detailed AP interview in March have now confirmed the clinical details. Twenty minutes of isolated speech loss. Painless. Clean imaging afterward. No diagnosis. These are no longer our inferences. They are first-person disclosures from the patient himself.
Twenty minutes of silence, 250 miles above the Earth. The voice came back. The explanation did not.
The next time it happens, Earth may not be close enough to matter.
Keep looking up.
-- The Sentinel
Sentinel Note: Every briefing we’ve published is free. That’s not changing. This publication has no institutional backing, no sponsors, and no editorial board. We’re doing the work the newsrooms won’t — sourcing papers, filing FOIAs, building tools, and writing at the pace a once-in-a-civilization event demands.
Paid subscribers fund the investigation directly. They also get access to the comment section on every briefing, Fieldcraft Labs, and the FIELDCRAFT series — the tools and methods behind every investigation we publish. No ads. No sponsors. No strings. Your subscription is a data point against the suppression gradient.
If you can’t subscribe, we don’t care. Read everything. Share everything. The mission is the mission.
If this briefing found you, someone shared it. If you think it matters, be that someone. The Sentinel runs on readers, not algorithms.
Subscribe to The Sentinel Network
Share this briefing. The Suppression Gradient documented what happens when this coverage reaches platforms that do not want you reading it. Every share, every restack, every forwarded link is a data point against the gradient.
Previous briefings: The Weigh-In | The Verdict | The Ancient Engine | The Curated Orbit | The Long Count | The Green Burial | The Dead Drop | The Ghost General | The Wide Angle | The Ignition Sequence | The Ghost Coma | The Heartbeat | The Surge | The Suppression Gradient | The Silent Edit | CONFIRMED: The TESS Contingency | The Three Days of Darkness | The Pacific Diversion | The Glomar Confirmation | The December Intersection | The SPHEREx Intercept | The Sentinel Dossier | Dossier 001
I'm an expert on this, and when they said he had lost his speech, I thought he had a stroke. I had a brain bleed almost 7 years ago. No pain. For the first 3 days afterward, I could only speak gobbledy-gook. On the 4th day my speech became normal...no treatment, and where my stroke occurred in my brain, surgery was not an option. There's more, but I'll leave it at that. Suffice to say...I shouldn't be here.
The questions are:
-Whether or not NASA screend him for a Patent Foramen Ovale after his return to earth?
-Whether NASA has gone ahead to screen all astronauts currently in their program?
-Whether they’ve added this screening to their protocols for qualifying future astronauts?